Every year June 25 is celebrated as the World Vitiligo Day to raise awareness regarding Vitiligo, fight prejudice, and raise funds for research, support & education. The aim of this day is to include the recognition of the bullying, social neglect, psychological trauma, and disability of millions of people affected by vitiligo. The primary purpose of this day is to raise money for research, give free skin exams, and educate physicians on how to best take care of patients with vitiligo.
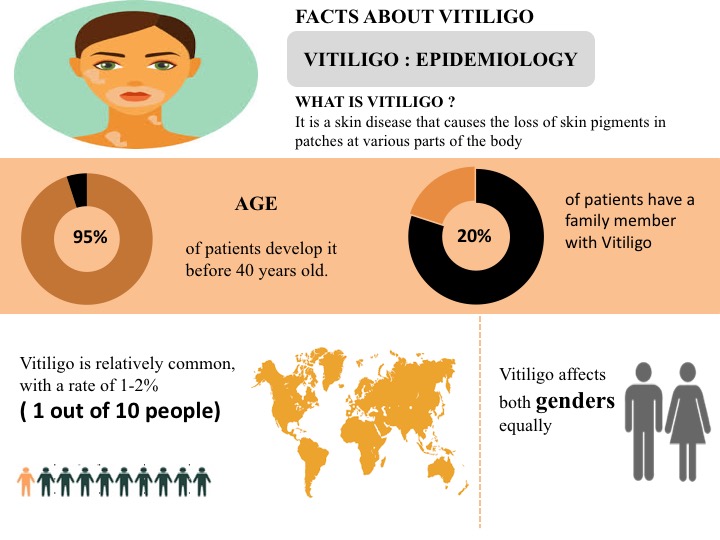
Vitiligo is the long term skin condition in which the skin loses the pigment i.e. melanin, essential for determining the color of skin, hair, and eyes. This leads to the slow growth of the white patches of irregular shapes on the skin. Vitiligo can also affect the mucous membranes, including tissues inside the mouth and nose. It can affect people of all skin types but is generally noticeable much in darker skin people.
Vitiligo Facts
Around 1 out of 10 people i.e. 1-2% of people are suffering from Vitiligo worldwide
The United States accounts for the highest prevalent cases of Vitiligo in comparison to the EU5 (Germany, France, Spain, Italy, and the United Kingdom) and Japan
Vitiligo is classified as the non-segmental, and segmental Vitiligo. Non-segmental Vitiligo is most prevalent in comparison to the segmental Vitiligo
Approximately, 95% of the people develop the condition prior to age 40.
Around 20% of people have a family member suffering from Vitiligo
Males and females are almost equally affected by Vitiligo
Vitiligo is sometimes associated with certain other medical conditions, including thyroid dysfunction, diabetes mellitus, Addison’s disease, etc.
Several factors such as autoimmune disease, genetic factors, sunburn or any cut, oxidative stress, neurochemicals, and exposure to the industrial chemicals increase the risk of developing Vitiligo
Myasthenia Gravis is a chronic autoimmune, neuromuscular disease that causes weakness in the skeletal muscles that worsens after periods of activity and improves after periods of rest. These muscles are responsible for functions involving breathing and moving parts of the body, including the arms and legs. It is characterized by muscular fatigue leading to extreme weakness. The fatigue is caused by the loss of ability to convert nerve impulses into muscle contraction. The disease affects muscles controlling voluntary movement including those associated with actions such as swallowing and breathing and usually begins in a mild form. Typical first symptoms are associated with the eyelid, sight, swallowing, and speech. Focal MG usually develops more or less rapidly into generalized MG with symptoms that appear in the arms and abdomen and subsequently in the legs and respiratory muscles.
Various diagnostic tests such as electro-diagnostics, diagnostic imaging, pulmonary function tests, and other tests are used for the diagnosis of Myasthenia Gravis. Thymectomy, Monoclonal antibody, Anticholinesterase medications, and Immunosuppressive drugs are recommended for the treatment of myasthenia gravis. Several pharmaceutical companies such as CuraVac, argenx BVBA, Cartesian Therapeutics, Momenta Pharmaceuticals, Inc., RemeGen, and others are involved in the development of novel therapies for the treatment of Myasthenia Gravis.
CuraVac (CV-MG01)
Myasterix (CV-MG01) is an investigational therapeutic vaccine being developed by Curavac to alleviate the symptoms of myasthenia gravis. Myasterix is likely to have fewer side effects and a simpler method of administration than other therapies. The Myasterix vaccine induces the body to produce a different type of antibody, which binds to autoantibodies and T-cell receptors associated with myasthenia gravis. Obstructing receptors of the anti-AChR T-cells with the Mysterix-produced antibody prevents autoimmune production of anti-AChR antibodies. This is expected to unblock the AChR, restoring neuromuscular communication via acetylcholine successfully binding to its receptor.
Myasterix, is currently investigated under a clinical trial study. The Study CV-0002 is the first clinical trial administering CV-MG01 in humans. This clinical trial is a safety and proof-of-concept study (proof of mechanism of action) intended to assess the safety, tolerability, and immunogenic response following three subcutaneous injections of CV-MG01 as a potential therapeutic vaccine / active immunotherapy in myasthenia gravis (MG) patients.
Argenx BVBA (ARGX-113/ Efgartigimod)
Efgartigimod is designed as a first-in-class investigational antibody fragment to target the neonatal Fc receptor (FcRn). Efgartigimod is being evaluated for the treatment of patients with severe autoimmune diseases with confirmed presence of pathogenic immunoglobulin G, IgG autoantibodies, where a severe unmet medical need exists.
Cartesian Therapeutics (Descartes-08)
Descartes-08 is a CD8+ CAR-T investigational therapy that targets cells expressing B-cell Maturation Antigen (BCMA), a protein expressed by all plasma cells. Descartes-08 is engineered to have a defined and predictable half-life, enabling repeat dosing to maximize potency while minimizing the risk of toxicity
UCB Biopharma S.P.R.L. (Rozanolixizumab)
Rozanolixizumab is a subcutaneously administered, humanized monoclonal antibody that specifically binds, with high affinity, to human FcRn. It has been designed to block the interaction of FcRn and IgG, inhibiting IgG recycling and inducing the removal of pathogenic IgG autoantibodies. Rozanolixizumab is under clinical development with the aim of improving the lives of people with pathogenic IgG-autoantibody-driven autoimmune diseases, including ITP, myasthenia gravis (MG) and chronic inflammatory demyelinating polyneuropathy (CIDP), by driving removal of pathogenic IgG autoantibodies
Momenta Pharmaceuticals, Inc.( M281/ Nipocalimab)
Nipocalimab (M281) is a fully human, anti-FcRn (neonatal Fc receptor), aglycosylated IgG1 monoclonal antibody. Nipocalimab (M281) has the potential of improving the clinical signs and symptoms of MG by blocking FcRn-mediated IgG recycling, thereby reducing pathogenic autoantibodies including the most common autoantibodies, anti-AChR and anti-MuSK. Nipocalimab, is investigated under clinical trial. The purpose of this study is to evaluate the safety, tolerability, and efficacy of M281 administered to participants with generalized myasthenia gravis (gMG) who have an insufficient clinical response to ongoing standard of care therapy.
Immunovant Sciences GmbH (IMVT-1401)
The investigational drug product candidate, IMVT-1401 (formerly known as RVT-1401), is a novel, fully human monoclonal antibody targeting the neonatal Fc receptor (FcRn). IMVT-1401 has the potential to address a variety of IgG-mediated autoimmune diseases as a subcutaneous injection. The FcRn receptor facilitates IgG recycling. IMVT-1401 enhances the degradation of IgG by targeting FcRn and preventing endogenous IgG from binding. This increased catabolism of IgG may curtail the harmful immune response exhibited by auto-antibodies.
Catalyst Pharmaceuticals, Inc. (Amifampridine Phosphate)
Amifampridine, a neuronal potassium channel blocker, is used for the treatment of MuSK-positive myasthenia gravis. Currently, Catalyst is enrolling patients into a phase III trial examining amifampridine for the treatment of Myasthenia Gravis. The MuSK Trial is a phase III, randomized, double-blind, placebo-controlled, parallel-group study evaluating the safety, tolerability, and efficacy of amifampridine in patients with MuSK-MG and a small sample of patients with AChR-MG. Amifampridine has received the Orphan Drug Designation from the Food and Drug Administration FDA for the treatment of patients with myasthenia gravis.
RemeGen (RC18)
Investigational candidate RC18 is a fusion antibody created by RemeGen scientists to target signaling factors involved in the development and survival of B cells, the cell responsible for generating antibodies. RC18 is a fusion of a TACI (transmembrane activator and calcium modulator and cyclophilin ligand interactors) protein and the IgG protein.
RC18 binds to BLyS (B lymphocyte stimulator) and APRIL (a proliferation-inducing ligand), preventing these cell-signaling molecules from binding to TACI proteins on the surface of the B cell. This inhibits the development and survival of mature B cells, preventing the formation of autoantibodies.
June is the Scoliosis Awareness Month that aims at highlighting the growing need for education, early detection, and awareness regarding scoliosis and its prevalence within the community. It unites scoliosis patients, families, physicians, clinicians, institutions, and related businesses in collaborative partnerships of local activities, events, and grassroots networking throughout the month.
Scoliosis Overview
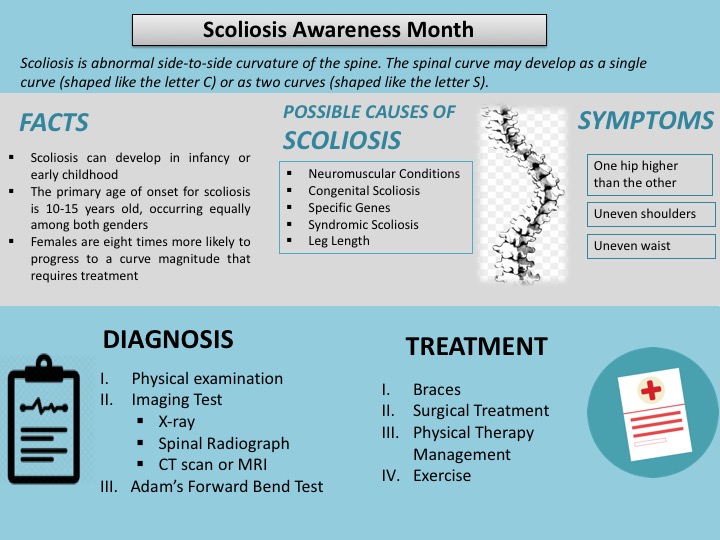
Scoliosis is an abnormal side-to-side curvature of the spine. The spinal curve may develop as a single curve (shaped like the letter C) or as two curves (shaped like the letter S). It is often defined as spinal curvature in the “coronal” (frontal) plane. While the degree of curvature is measured on the coronal plane, scoliosis is actually a more complex, three-dimensional problem which involves the following planes:
Coronal plane
Sagittal plane
Axial plane
The coronal plane is a vertical plane from head to foot and parallel to the shoulders, dividing the body into anterior (front) and posterior (back) sections. The sagittal plane divides the body into right and left halves. The axial plane is parallel to the plane of the ground and at right angles to the coronal and sagittal planes.
Scoliosis is hereditary among the people with scoliosis who are more likely to have children with scoliosis; however, there is no correlation between the severity of the curves from one generation to the next. In children and teens, scoliosis often does not have any noticeable symptoms and may not be noticeable until it has progressed significantly. Most cases of scoliosis are mild, but some spine deformities continue to get more severe as children grow. Severe scoliosis can be disabling. An especially severe spinal curve can reduce the amount of space within the chest, making it difficult for the lungs to function properly. The most common form of scoliosis appears in adolescents. It is known as adolescent idiopathic scoliosis. It can affect children from the age of 10 years.
The symptoms can include the head is slightly off center, the ribcage is not symmetrical, so the ribs may be at different heights and one hip is more prominent than the other. Furthermore, in infants, symptoms can include: a bulge on one side of the chest, consistently lying curved to one side (in babies), Problems with the heart and lungs, leading to shortness of breath and chest pain.
According to the American Association of Neurological Surgeons (AANS), about 80 percent of scoliosis cases have no identifiable cause. The condition is often diagnosed during the first seven years of a child’s life.
Etiology
Neuromuscular Conditions: These affect the nerves and muscles and include cerebral palsy, poliomyelitis, and muscular dystrophy.
Congenital Scoliosis (present at birth): This is rare and occurs because the bones in the spine developed abnormally when the fetus was growing inside the mother.
Specific genes: At least one gene is thought to be involved in scoliosis.
Leg length: If one leg is longer than the other, the individual may develop scoliosis.
Syndromic scoliosis: Scoliosis can develop as part of another disease, including neurofibromatosis and Marfan’s syndrome.
Osteoporosis: This can cause secondary scoliosis due to bone degeneration.
Risk Factors
There are certain risk factors associated with scoliosis include: age, gender & genetics etc. are explained below:
Age: Signs and symptoms often start during a growth spurt just before puberty.
Gender: Females have a higher risk in comparison to the males
Genetics: People with scoliosis may have a close relative with the condition.
Diagnosis
Scoliosis is confirmed through a physical examination, an x-ray, spinal radiograph, CT scan or MRI. The curve is measured by the Cobb Method and is diagnosed in terms of severity by the number of degrees. A positive diagnosis of scoliosis is made based on a coronal curvature measured on a posterior-anterior radiograph of greater than 10 degrees. In general, a curve is considered significant if it is greater than 25 to 30 degrees. Curves exceeding 45 to 50 degrees are considered severe and often require more aggressive treatment.
A standard exam that is sometimes used by pediatricians and in grade school screenings is called the Adam’s Forward Bend Test. During this test, the patient leans forward with his or her feet together and bends 90 degrees at the waist. This is a simple initial screening test that can detect potential problems, but cannot determine accurately the exact type or severity of the deformity. The tests are required for an accurate and positive diagnosis.
Physical Examination
Doctor would check the spine curvature and whether the shoulders and waist area are symmetrical or not.
Imaging Tests
Imaging tests doctor may order to look for scoliosis include:
X-ray: During this test, small amounts of radiation are used to create a picture of your spine.
MRI scan: This test uses radio and magnetic waves to get a detailed picture of bones and the tissue surrounding them.
CT scan: During this test, X-rays are taken at a variety of angles to get a 3-D picture of the body.
Bone scan: This test detects a radioactive solution injected into your blood that concentrates in areas of increased circulation, highlighting spinal abnormalities.
Treatment
Treatment of scoliosis is based on the severity of the curve and the chances of the curve getting worse. Certain types of scoliosis have a greater chance of getting worse, so the type of scoliosis also helps to determine the proper treatment. There are three main categories of treatment i.e. observation, bracing (for example, thoracolumbosacral orthosis or TLSO back brace), and surgery. Consequently, there are treatments available that do not involve surgery, but in some individuals, surgery may be their best option.
Observation
In many children with scoliosis, the spinal curve is mild enough to not require treatment. However, if the doctor is worried that the curve may be increasing, he or she may wish to examine the child every four to six months throughout adolescence.
In adults with scoliosis, X-rays are usually recommended once every five years, unless symptoms are getting progressively worse.
Bracing
Braces are only effective in patients who have not reached skeletal maturity. If the child is still growing and his or her curve is between 25 degrees and 40 degrees, a brace may be recommended to prevent the curve from progressing. There have been improvements in brace design and the newer models fit under the arm, not around the neck. There are several different types of braces available. For optimal effectiveness, the brace should be checked regularly to assure a proper fit and may need to be worn 16 to 23 hours every day until growth stops.
Surgery
In children, the two primary goals of surgery are to stop the curve from progressing during adulthood and to diminish spinal deformity. Most experts would recommend surgery only when the spinal curve is greater than 40 degrees and there are signs of progression. This surgery can be done using an anterior approach (through the front) or a posterior approach (through the back) depending on the particular case.
A number of factors can lead to increased surgical-related risks in older adults with degenerative scoliosis. These factors include the following: advanced age, being a smoker, being overweight and the presence of other health/medical problems. In general, both surgery and recovery time are expected to be longer in older adults with scoliosis.
Following surgical procedures are used for the treatment of scoliosis
Posterior approach: The most frequently performed surgery for adolescent idiopathic scoliosis involves posterior spinal fusion with instrumentation and bone grafting. This is performed through the back while the patient lies on his or her stomach.
Anterior approach: The patient lies on his or her side during the surgery. The surgeon makes incisions in the patient’s side, deflates the lung and removes a rib in order to reach the spine. Video-assisted thoracoscopic (VAT) surgery offers enhanced visualization of the spine and is a less invasive surgery than an open procedure. The anterior spinal approach has several potential advantages: better deformity correction, quicker patient rehabilitation, improved spine mobilization and fusion of fewer segments.
Decompressive laminectomy: The laminae (roof) of the vertebrae are removed to create more space for the nerves. A spinal fusion with or without spinal instrumentation is often recommended when scoliosis and spinal stenosis are present. Various devices (like screws or rods) may be used to enhance fusion and support unstable areas of the spine.
Minimally invasive surgery (MIS) : Fusion can sometimes be performed via smaller incisions through MIS. The use of advanced fluoroscopy (X-ray imaging during surgery) and endoscopy (camera technology) has improved the accuracy of incisions and hardware placement, minimizing tissue trauma while enabling a MIS approach. It is important to keep in mind that not all cases can be treated in this manner and a number of factors contribute to the surgical method used.
The benefits of surgery should always be weighed carefully against its risks. Although a large percentage of scoliosis patients benefit from surgery, there is no guarantee that surgery will stop curve progression and symptoms in every individual.
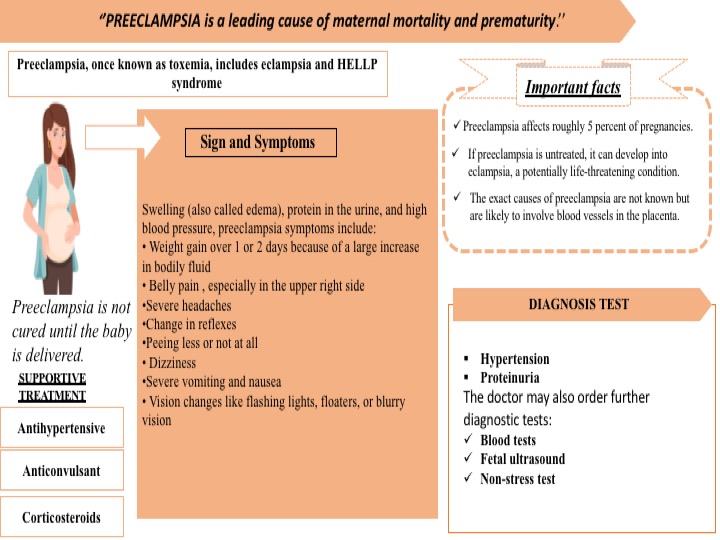
Pre-eclampsia is a leading cause of maternal mortality and prematurity. It is formerly called toxemia, which is when a pregnant woman has high blood pressure, protein in her urine, and swelling in her legs, feet, and hands. It can range from mild to severe. It usually happens late in the pregnancy after 20 weeks of pregnancy, though it can come earlier or just after delivery. In addition, there are several complications associated with preeclampsia such as HELLP syndrome, poor blood flow to the placenta & placental abruption, etc. Preeclampsia can lead to eclampsia, a serious condition that can have health risks for mom and baby and, in rare cases, cause death. Women with preeclampsia who have seizures have eclampsia. Approximately around 5% of all pregnant women get affected by preeclampsia.
The symptoms often begin after 34 weeks. Symptoms develop after birth, usually within 48 hours of delivery in few cases. They tend to go away on their own but can last up to 12 weeks after birth. In addition, the common symptoms develop such as edema, protein in the urine, and high blood pressure, preeclampsia symptoms include weight gain, belly pain, severe headaches, changes in reflexes, peeing less or not at all, dizziness, severe vomiting and nausea, vision changes like flashing lights, floaters, or blurry vision
Yet, the exact cause of preeclampsia is unidentified. But most of them say this problem happens with the development of the placenta because the blood vessels that supply it are narrower than normal and respond differently to hormonal signals. Because the blood vessels are narrower than normal, blood flow is limited. Several factors such as the history of preeclampsia, age, race, chronic hypertension, first pregnancy, obesity, and multiple pregnancies increase the chances of developing the preeclampsia
Preeclampsia is diagnosed through the following tests:
Hypertension: The woman’s blood pressure is raised above 140/90 millimeters of mercury is abnormal in pregnancy.
Proteinuria: Protein is detected in the urine is indicated for the severity of the condition.
The doctor may also recommend some further diagnostic tests:
Blood tests – to assess the kidney and liver functions.
Fetal ultrasound – to monitor the baby’s progress.
Non-stress test – the doctor checks how the baby’s heartbeat reacts when they move. If the heartbeat increases 15 beats or more a minute for at least 15 seconds twice every 20 minutes, it is an indication that everything is normal
Recently, UniSA biomedical engineer Professor Benjamin Thierry developed a range of solid-state sensing and wearable technologies capable of diagnosing conditions including preeclampsia, epilepsy, fetal arrhythmias, and heart attacks. These wearables use a cutting-edge solid-state sensing technology called Field-Effect Transistors, which can measure bioelectric signals with extreme sensitivity when implemented at the nanoscale.”
However, Preeclampsia is not cured until the baby is delivered. Hence, the mother’s blood pressure comes down, she is at a greater risk of stroke, severe bleeding, separation of the placenta separates from the uterus and seizures. In some cases, especially if the preeclampsia started early, the delivery may not be the best option for the fetus.
Supportive therapy is recommended for the women Preeclampsia. Supportive therapy is as follows:
Antihypertensives: These are used to lower blood pressure.
Anticonvulsants: In severe cases, these drugs are used to prevent a first seizure. The doctor may prescribe magnesium sulfate.
Corticosteroids: If the mother has preeclampsia or HELLP syndrome (see below) these drugs can improve platelet and liver functioning. This can prolong pregnancy.
While preeclampsia cannot be fully prevented, there are significant steps a woman can follow to avoid the moderate factors contribute to high blood pressure.
These may include:
drinking between 6 and 8 glasses of water every day
avoiding fried or processed food
excluding added salt from the diet
regular exercise
avoiding alcohol and caffeine intake
keeping the feet elevated a few times per day
resting
supplements and medications as prescribed by your doctor